Which is the “correct” term: Alzheimer’s disease, Alzheimer disease? Should the eponym be replaced entirely?
According to the Wikipedia article on medical eponyms, “medical eponyms are terms used in medicine which are named after people (and occasionally places or things). In 1975, the Canadian National Institutes of Health held a conference that discussed the naming of diseases and conditions. This was reported in The Lancet where the conclusion was summarized as: “The possessive use of an eponym should be discontinued, since the author neither had nor owned the disorder”. New discoveries are often attached to the people who made the discovery because of the nature of the history of medicine.”
The existence of multiple terms to refer to the same concept/disease in medicine, or conversely, the same word being used to mean absolutely unrelated concepts, creates an inconvenience in medicine. This is most evident in database probes. If a person were to do a database probe on a particular disease or concept, he would need to incorporate all the different terms used to refer to that particular concept (e.g. searching for McArdle’s disease, you would probably have to include the term “glycogen storage disease type V” too for a truly rigorous and comprehensive search).
As the search results roll out, he would then need to be cautious not to waste time on the search results which have mainly incorporated the alternative meanings of the desired term (e.g. Purkinje fibres associated with the cardiac conduction system are absolutely different from the Purkinje neurons in the cerebellum).
Let’s not even get started on the differences in American English and British English (oestrogen vs. oestrogen) and the arbitrary use/lack of use (e.g. Type V vs. Type 5) of Roman numerals which create even more hassle in rigorous database searches. Furthermore, generic names for drugs/hormones may be different from the US and that of the rest of the world (e.g. paracetamol vs. acetaminophen; salbutamol vs. albuterol; adrenaline vs. epinephrine). Here is the skeletal formula of paracetamol:

Fun fact: Paracetamol and acetaminophen both derive from the systematic chemical name for the drug: N-acetyl-para-aminophenol. To get either term, different parts of the chemical name were taken and compounded to yield a new generic drug term!
In my first semester last year, I had a physiology assignment which consisted of several questions, the first of which pertained to the pathophysiology of Tay-Sachs disease, a lysosomal storage disease. As with the names of many diseases/syndromes/disorders, this was yet another eponym. Usually, when we come across diseases with eponyms, we often think that eponyms are perhaps the surname(s) of the men who have been the first to document the said disease. In most cases, this would be true.
However, in some cases, the eponym is associated with the patient who suffered from the disease (e.g. Christmas disease, Hartnup disease), or even a location (e.g. Lyme disease, Marburg virus). Lyme disease was named after its namesake, a small coastal town in Connecticut, a state in the US, where in 1975, a woman brought an unusual cluster of paediatric arthritis cases to the attention of Yale researchers. In 1977, the Yale researchers identified and named the clusters Lyme arthritis.
As I studied the glycogen storage diseases and lysosomal storage diseases a few months ago, I couldn’t help but notice that virtually all the diseases had medical eponyms.
Off the cuff, at least for the more prominent lysosomal storage disorders, all but one I can think of are all eponyms. Consider this diagram:
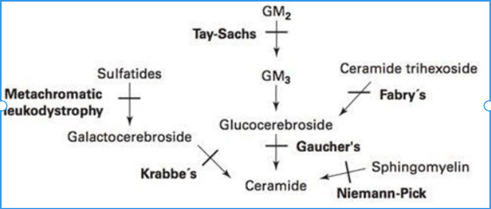
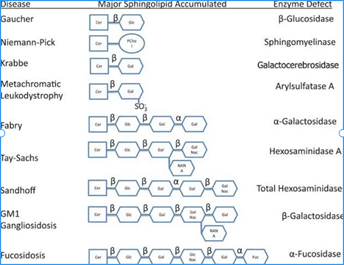
And the above is only for the diseases implicating sphingolipids (i.e. sphingolipidoses). Another category of lysosomal storage diseases would be the mucopolysaccharidoses, the most prominent of which are Hurler’s syndrome and Hunter’s syndrome. Only metachromatic leukodystrophy isn’t an eponym! Here is another useful image I found that shows you how deficiencies of various enzymes in sphingolipid metabolism result in the accumulation of various sphingolipid derivatives:
In fact, a few months ago, I had a chat with my friend who is a doctor. I told her something along the lines of “many diseases are due to deficiencies in particular enzymes. Instead of having these eponyms, wouldn’t it be easier if the common name for all these diseases took the form: “[enzyme name] + deficiency”? The name would then provide functionally useful information. What use is knowing that two men with surnames Tay and Sachs helped document Tay-Sachs disease? Its alternative names: Hexosaminidase A deficiency, and GM2 gangliosidosis tell us so much more!”
We just laughed, and chuckled at such a quixotic notion. After all, one does not simply just go about and casually dictate the conventions and traditions to which the medical fraternity chooses to adhere.
For the glycogen storage diseases, which have many types, types I, II, III, IV, V, VI, VII are von Gierke’s, Pompe’s, Cori’s, Andersen’s, McArdle’s, Hers’, and Tarui’s, respectively. There are also sub-types and other types which are rarer. Today, at least 15 types of GSDs have been documented.
One possible explanation for the survival of some eponyms despite the existence of functionally useful alternative terms is that the eponyms are coined before the pathophysiology of the disease could be worked out. This is not surprising because usually, one would expect that the clinical signs and symptoms are documented first. It is only thereafter that research is conducted to find out more. In the case of Tay-Sachs, the root cause of Hexosaminidase A deficiency was only discovered in 1969, long after British ophthalmologist Dr Warren Tay initially described the characteristic cherry-red spots seen on one of his patients’ retina in 1881.

NB: Cherry-red spots on the macula are also seen in Niemann-Pick’s disease; the way to differentiate between the two diseases is via the presence/absence of hepatosplenomegaly in Niemann-Pick and Tay-Sachs, respectively.
That’s the way medicine is. The medical fraternity appears to relish its long-standing traditions. Anecdotally, I think many senior physicians would be more comfortable with the use of eponyms. This is in contrast with the recent trend of not favouring eponyms. People who discourage the use of eponyms have the following arguments:
1. “They don’t reflect the pathophysiology”. I have already covered this with the example of Tay-Sachs disease above. In many cases, there is simply little you can do about it. For many eponyms, especially for those of common diseases, the eponyms are so widely used that using the alternative terms would do you inconvenience and a disservice to yourself and your peers. You would probably be asked to clarify yourself if you insist on using a term that is not commonly used. This is a major reason I suspect that the US would likely never use the metric in practice. The economic cost simply doesn’t justify it, and even if there were economic aspect of the problem were resolved, people are simply too accustomed to the status quo. In the case of the imperial units which the US uses, whole institutions in that vast country have been established and worked on the premise of the imperial units. Enforcing a change of units would likely cause unbelievably great inconvenience to many people. Likewise, we see a similar phenomenon with medical eponyms. Even if an alternative term makes “more sense” to you, there is no point using it if your peers are just going to seek clarification all the time.
2. They may stigmatise certain groups of people. Did you know that syphilis used to be termed the “French disease”? According to its Wikipedia article, the first written records of an outbreak of syphilis in Europe occurred in 1494 or 1495 in Naples, Italy, during a French invasion (Italian War of 1494-8). Since it was claimed to have been spread by French troops, it was initially called the French disease by the people of Naples. The French should be glad that syphilis no longer adopts its former name as it would only add to the list of stereotypes that people have of them!
3. They may glorify people associated with undesirable and shunned ideologies. Believe it or not, there is actually a Wikipedia page on medical eponyms associated with the Nazis (see reference [4]). Of this subset of medical eponyms, Asperger’s syndrome is probably the most well-known. The syndrome is named after Hans Asperger who apparently “managed to accommodate himself to the Nazi regime and was rewarded for his affirmations of loyalty with career opportunities.” He “joined several organisations affiliated with the Nazi party, though not with the Nazi party itself, and publicly legitimized race hygiene policies including forced sterilizations and, on several occasions, actively cooperated with the child ‘euthanasia’ program.” Despite this history, Asperger remains honoured in the form of the eponym partially because his involvements with the Nazis were not so direct and notable, in stark contrast with some other physicians (you’ll never hear Mengele getting honoured with an eponym).
While learning respiratory physiology and histology, I chanced upon Club cells (formerly known as Clara cells):

Club/Clara cells are nonciliated cells, as you can see from the above illustration. Clara cells are located in bronchioles and the functions of these cells include: 1) degrading toxins, 2) secreting a component of the pulmonary surfactant, 3) acting as reserve cells.
This “Clara” wasn’t the name of a woman. It was the surname of Dr Max Clara, who according to the relevant Wikipedia article: “was an active member of the Nazi Party and used tissue taken from executed victims of the Third Reich for his research—including the work that led to his discovery of Clara cells. In May 2012, the editorial boards of most of the major respiratory journals (including the journals of the American Thoracic Society, the European Respiratory Society and the American College of Chest Physicians) concluded that the continued use of Clara’s eponym would be equivalent to honoring him; they therefore introduced a name-change policy, which went into effect beginning January 1, 2013. The term “Clara” was used parenthetically after “club cell” for a 2-year period, after which “Clara cell” and “Clara cell secretory protein” were conclusively replaced with “club cell” and “club cell secretory protein”, respectively.
Who knew that such innocent terms would have such a backstory? I once mentioned this to a friend whose name is Clara. Maybe she’ll discover something else and have something named after her!
As we have seen above, there are various reasons that people wish to stop using medical eponyms in certain scenarios. Nevertheless, I am personally in favour of eponyms, as I opine that the merit warranted by the following factors outweigh the disadvantages associated with eponyms.
1. They favour communication, and are definitely more succinct than equivalent descriptive terms, which are usually longer. It could also potentially be the case that there isn’t any satisfactory alternative descriptive term because the symptoms may be too broad, or not enough is known about the disease, etc.
2. They distinguish between different forms of a particular symptom/concept, thus allowing for more accurate description (e.g. Sydenham’s chorea vs. Huntington’s chorea).
3. They may commemorate the achievements of hardworking doctors, patients, and other medical staff whose contribution may otherwise be lost to posterity. They also give recognition to otherwise relatively unknown places (e.g. Lyme disease, Marburg virus).
4. This is an important counterargument to the earlier point on how eponyms may stigmatise certain groups of people. In fact, one classic example of how eponyms help people reduce stigmatisation is the case of leprosy. The general public would be well-acquainted with leprosy, but its eponym is much less familiar to the layperson: Hansen’s disease. Eponyms can also help preserve patient dignity (e.g. Angelman’s syndrome vs. Happy Puppet Syndrome) and avoid racism (e.g. Down’s syndrome vs. Mongolism).
5. Eponyms pique the curiosity of those who are interested in the history of a disease or a concept. They teach us about medical history and culture: the noble work that our forefathers have done to give us the immense cumulative wealth of medical knowledge that we have today. In some cases, the eponyms tell us an amusing story! For instance, Professor Sir Edwin Southern (who is still alive) invented the Southern blot procedure in 1975, a procedure that is commonly used in laboratories today for detection of a specific DNA sequence in DNA samples. Following this invention, the Northern and Western blots were developed as blotting procedures which involved RNA and proteins, respectively. Clearly, you can see the play on words! This naming convention on directionality wouldn’t have happened if not for the initial Southern eponym and at least one other biologist’s sense of humour!
NB: A helpful mnemonic for the various blots and the substances is: SNoW DRoP, where S, N, and W are Southern, Northern, Western, and D, R, and P are DNA, RNA, and Protein respectively!
In fact, what do you think a Southwestern blot entails? If you guessed that it’s something that involves both DNA and proteins, then congratulations! You’ve just demonstrated how marvellous eponyms can be! Southwestern blots identify DNA-binding proteins!
6. If we’re being honest with ourselves, these eponyms often make us sound more sophisticated. Which is more sophisticated – noting the four symptoms: pulmonary infundibular stenosis, right ventricular hypertrophy, overriding aorta, ventricular septal defect, or elegantly presenting it simply as “Tetralogy of Fallot”? Evidently, the latter is more succinct.
What do you think of eponyms? Let me know your thoughts!
Yours faithfully,
NL
20 September 2019
References & Further Reading
1. https://www.bmj.com/content/349/bmj.g7586
2. https://www.ntsad.org/index.php/tay-sachs/history
3. https://en.wikipedia.org/wiki/Syphilis
4. https://en.wikipedia.org/wiki/List_of_medical_eponyms_with_Nazi_associations
5. https://en.wikipedia.org/wiki/Club_cell#Clinical_significance
6. https://en.wikipedia.org/wiki/Southern_blot
7. https://bitesizebio.com/639/southern-northern-western-and-eastern/

Leave a comment