On Friday, I concluded my three-week stint at Queenstown Polyclinic as part of the ten-week Family Medicine (FM) posting of the third year of the NUS MBBS undergraduate curriculum (i.e. Phase III). There were various assessment components associated with this three-week stint, one of which was the ‘patient care plan’ that each medical student was expected to complete.
I decided to craft a care plan for an 86-year-old woman whom I had the privilege of encountering during the polyclinic attachment. I could spend time talking about all the various aspects of her care but for the purposes of this post, I would like to talk about how I have witnessed first-hand the importance of managing chronic diseases, and knowing the various nuances in the current guidelines so that we can deliver evidence-based care for the good of our patients.
Singapore’s population is ageing, and it is indeed staggering to see for myself the sheer proportion of patients who visit the polyclinic (particularly for chronic consults) who present with a personal medical history of the common chronic diseases: hypertension, diabetes mellitus, hyperlipidaemia, osteoarthritis. Unfortunately, the statistics on the predicted trends on the prevalence and incidence of these diseases paint a bleak picture.
As the average life expectancy increases (age is a classic non-modifiable risk factor for many chronic diseases) and the proliferation of the modern diet (which is generally unhealthy, processed, and laden with added sugar, particularly high fructose corn syrup) continues without bounds, both the prevalence and incidence of these chronic diseases are going to rise.
Why is this a concern? Let’s take one of the chronic diseases, diabetes mellitus (DM), for example. In the case of DM, complications can be classified as acute (hyperglycaemia symptoms, and hypoglycaemia symptoms secondary to DM therapy) and chronic. Chronic complications can be classified as microvascular (e.g. diabetic retinopathy, diabetic neuropathy, diabetic nephropathy) and macrovascular (stroke, acute coronary syndrome, peripheral vascular disease). In addition to the decreased quality of life experienced by the individual in view of all the potential complications, there is a real tangible cost to society: the cost of the medical services and resources deployed to diagnose DM, manage DM, etc. How can we keep healthcare costs reasonably low without compromising on accessibility and quality? This problem is exacerbated by the fact that Singaporeans aren’t keen on having children (c.f. data from Singapore’s 2020 census). So, where exactly are we going to find the means to pay for the increasing healthcare expenditure associated with an ageing population?
I have heard a lot about how prevention is better than cure, and that we need to win the war on diabetes, etc. These concepts are great. However, they can be rather abstract if one is not affected by these chronic diseases or personally knows loved ones, peers, friends, and colleagues who are affected by these chronic diseases. Having seen so many patients and their journey with chronic diseases has made me come to the realization that indeed, prevention truly is better than cure. It’s much more cost-effective too. But even if one has been diagnosed with a chronic disease, all hope is not lost. This is because chronic diseases can be managed!
In the specific case of the 86-year-old patient I had encountered, I had the following takeaways:
1) There is a lot more to target control than just adhering to the doctor’s management plan. Positive health outcomes are not guaranteed even if patients adhere to the plan established by their doctors, and this is because there are other factors that are (at least in 2021) beyond the control of both the patient and the doctor. Despite being 86yo, and having reported dietary indiscretion, her glycaemic and lipid control are excellent. She isn’t exactly on intense drugs, and she doesn’t even do home blood pressure monitoring (HBPM). In stark contrast, I have seen many patients who are younger than her. These patients may be more disciplined in their lifestyle habits, adhere more to the doctor’s management plan, are on stronger drugs, and still do not achieve values as good as her. As such, genetics plays a huge role. As with virtually all major diseases, the interplay between genetics and environmental factors is significant and we must always bear that in mind. If patients have sincerely tried their best and are still unable to meet certain health targets, we should graciously accept the situation for what it is and not fault them for things beyond their control. On the other hand, having favourable genetic disposition is not an excuse for poor adherence to the prescribed management plan.
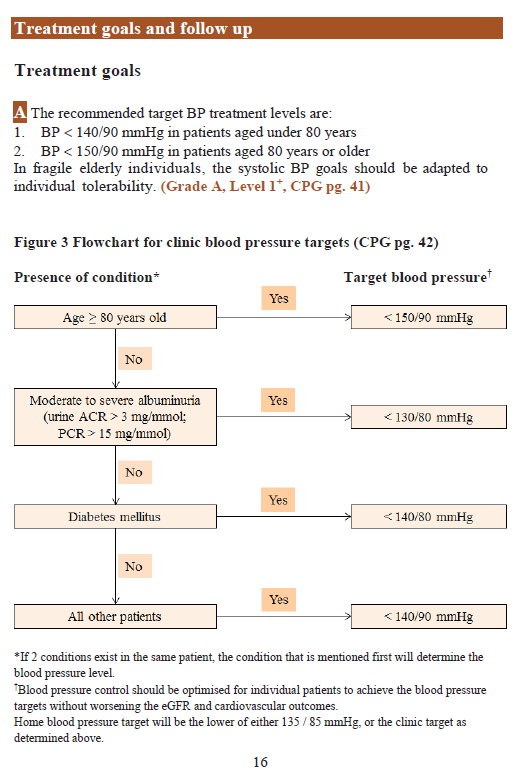
2) I have learnt the importance of personalised targets for particular subset of patients. For example, in patients who are aged 80 years or older, the blood pressure target is no longer as strict and becomes 150/90. The age-associated BP target change takes precedence.
As for the hypothetical patient’s ideal HbA1c target, although we like to throw the 7% number around a lot out of convenience, the reality is that the ideal HbA1c target should be individualised to the patient’s biodata, DM history, and comorbidities. As such, with the 86-year-old patient’s profile, an appropriate target would be an HbA1c% target of 7.5%. The HbA1c% target may be as low as 6.5% in young and healthy patients while it may be 8.0% in very old patients with highly advanced DM. So, chronic management of DM requires a multidisciplinary holistic management centred around patient education to meet individualised glycaemic targets with non-pharmacological and pharmacological means while simultaneously managing complications and comorbidities. The same reasoning (i.e. in the previous sentence of this paragraph) could be applied to other chronic diseases; just change the phrase ‘individualised glycaemic targets’ to something relevant for the chronic disease in question.
In summary, this case, and the process of putting together the care plan for the 86-year-old patient as a practice exercise have constituted an excellent opportunity for me to understand first-hand the reality of chronic disease management in Singapore. It is certainly not easy at all, particularly if one truly wants to ensure that the management plan is personalised in the name of evidence-based practice. As mentioned earlier, the trends on diabetes prevalence (and similarly for other chronic diseases) don’t look particularly promising. As such, for most of us who will be doctors in the primary care setting, we need to be mentally prepared to manage an ever-increasing proportion of patients with chronic diseases.
NL
26 September 2021

Leave a comment