What a ride it has been. I just concluded the penultimate week of the Year 3 Family Medicine (FM) posting. Specifically, I just completed the second of two weeks of the GP component of the FM posting, and I must say that the fortnight that I have spent here at this clinic has been the most meaningful fortnight I have encountered yet in this academic year.
For GP attachments, students are posted to doctors in pairs. My clinical group partner and I were fortunate to have been posted to this particular GP clinic in Sengkang, which relishes a decent patient load. The doctor possesses an excellent reputation, and it is not hard to see why. After sitting in just the first few consultations that he had with his patients, I realise that he goes the extra mile to get patients personally involved in their care. The advice he gives patients is also personalised (giving specific personalised weight loss targets) and appreciated by many patients. Allow me to elaborate on what I mean.
The GP keeps his handy physical copy of the eighth edition of Dr John Murtagh’s Patient Education in his clinic. Towards the end of each consultation session, with respect to patient advice, he would flip to the relevant pages in the book, and ask them to take a photo of the relevant page(s) with their phone so that they can benefit from further reading even after the consultation has ended. This arrangement is beneficial for multiple reasons. Firstly, the amount of time available for the doctor to provide personalised patient education is limited in the typical GP clinic. This is unlike the case in polyclinics, where there may be an advanced practice nurse who dispenses patient education advice. Providing patient education via an esteemed book such as Murtagh’s Patient Education is a reasonable alternative. For the time saved by this arrangement, the doctor is able to see more patients, solve more issues for more people in the same limited amount of time, and also generate more revenue for the clinic.
In addition to allowing his patients to take a photograph of relevant pages in Patient Education, this GP also has his own leaflets of patient education that he personally prepares beforehand: leaflets that he would hand to the patients. He prepares these leaflets via Microsoft Word, and prints multiple copies to be stored in the clinics. He has a leaflet for every commonly encountered problem in the primary care setting (e.g. fever in children, diarrhoea, constipation, gastro-oesophageal reflux disease, gastritis). These leaflets provide a short definition of the disease entity, common aetiologies, clinical features, and advice on how the patient can do his part in the management of the condition. For example, in one such leaflet on gastro-oesophageal reflux disease, I remember seeing under one section how patients are advised to sleep in a left lateral decubitus position with their head elevated, while also avoiding triggers such as chocolate, caffeine, tea, spicy foods in general, and food and liquid consumption in the hours just preceding nocturnal slumber. Having a section on Dos and Don’ts for patients is practical and useful because it directly assures patients on practical steps they can take to manage their condition in conjunction with their doctor. By extension, patients may feel that they play an important part in their recuperative journey, and this can have positive downstream effects on future patient adherence.
Hopefully, the above has provided sufficient background and context for what I have undergone the past fortnight.
During the afternoon session of the clinic on Thursday, a Chinese male middle-aged smoker came in for an initial consult with the doctor. While the GP was conversing with his patient for an unrelated matter, I noticed a Hutchinson’s sign of the nail on the patient’s right third toe, which was accompanied by ulceration and partial nail plate destruction. Imagine if the patient had worn closed-toe shoes. I would not have picked it up. Thank God I happened to be observant. So, what is Hutchinson’s sign of the nail?
As discussed in an earlier blog post on eponyms, eponyms are ubiquitous in medicine. It particularly doesn’t help when the same eponym is used to refer to different phenomena within medicine, thus necessitating the use of additional clarifying identifiers. In the case of this specific “Hutchinson’s sign”, we require the additional “of the nail” to distinguish it from the following:
- Hutchinson‘s sign of the pupil
- A mydriatic and unreactive pupil on the same side of the body as an ipsilateral intracranial mass
- Hutchinson‘s sign of the nose
- Vesicles on the nasal tip, the lateral aspects of the nose, both of which may precede the development of herpes zoster ophthalmicus, also known as ophthalmic zoster or ophthalmic shingles
- NB: herpes zoster ophthalmicus is different from herpes zoster oticus, which is the entity perhaps better known by the eponymous ‘Ramsay-Hunt syndrome’)

- Hutchinson triad, a triad pathognomonic of congenital syphilis which consists of interstitial keratitis (NB: keratitis refers to inflammation of the cornea; the word “interstitial” reminds us that it is specifically the stromal layer, the thickest of the five layers of the cornea, which is inflammed), malformed teeth (which includes Hutchinson incisors and Mulberry molars), and sensorineural hearing loss
We have the late Sir Jonathan Hutchinson to thank for all the above eponyms. Anyway, a positive Hutchinson’s sign of the nail should raise one’s suspicions for a subungual (‘ungium‘ is the Latin word for ‘nail’; by extension, ‘subungual‘ refers to ‘underneath the nail‘) melanoma, a subtype of acral lentiginous melanoma, which itself is a type of malignant melanoma.
For readers who are not in the medical field, this can all sound like Greek. So, for the sake of accessibility, let’s first establish a basic mental model about skin cancers. When we talk about skin cancers, we can categorise them as non-melanomas (NMSC; cancers grouped under this term are considered benign simplistically because they are much less likely than malignant melanomas to spread and have serious adverse effects on the patient) or malignant melanomas. There are many different types of malignant melanoma, of which the more common ones include superficially spreading melanoma, nodular melanoma, lentigo maligna, and acral lentiginous melanoma. While homing in on the acral lentiginous type of melanoma, let’s try to understand some of the big words here.
The word ‘acral’ is defined as ‘of or belonging to the extremities of peripheral body parts’. The word ‘lentiginous’ comes from the word ‘lentigo’, which is a dermatological term used to describe a small pigmented lesion that is clearly demarcated from surrounding healthy skin. I find the following elaboration on ‘lentiginous’ from Wikipedia quite helpful and educational:
It is a harmless (benign) hyperplasia of melanocytes which is linear in its spread. This means the hyperplasia of melanocytes is restricted to the cell layer directly above the basement membrane of the epidermis where melanocytes normally reside. This is in contrast to the “nests” of multi-layer melanocytes found in moles (melanocytic nevi). Because of this characteristic feature, the adjective “lentiginous” is used to describe other skin lesions that similarly proliferate linearly within the basal cell layer.
Wikipedia
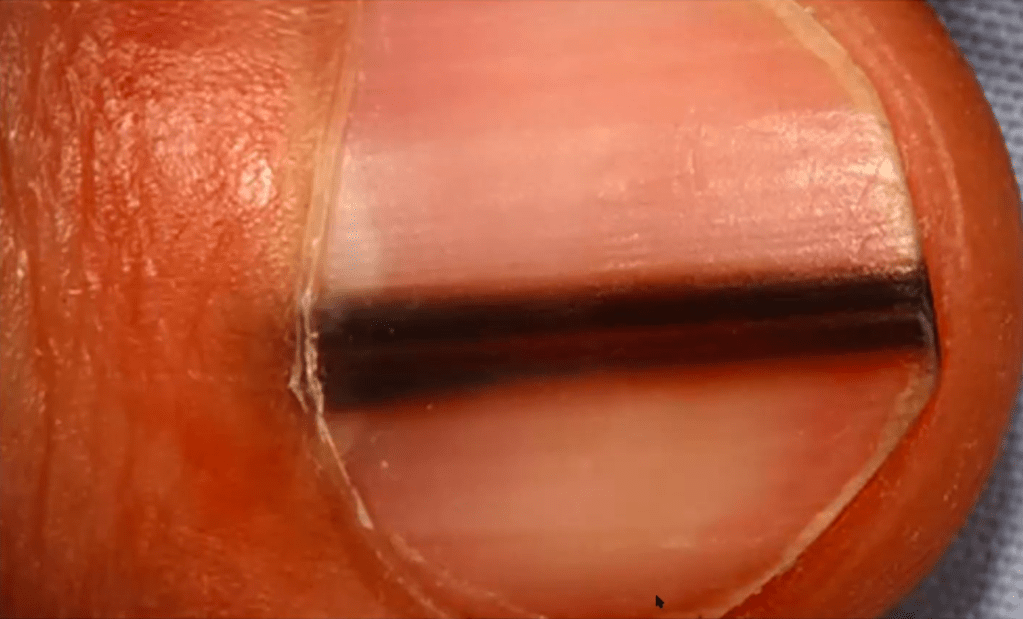
Acral lentiginous melanoma accounts for about 5% of all melanomas, and is more common in Asians and dark-skinned populations. Predilection sites in acral lentiginous melanoma include unsurprisingly (as the word ‘acral’ suggests) the palms, soles, the nail bed, and the mucous membranes. The following image is an example of Hutchinson’s sign of the nail, which constitutes the classic clinical appearance of the subungual subtype of acral lentiginous melanoma. According to the AMBOSS Knowledge library, Hutchinson’s sign of the nail is a dark linear patch, which arises from the proximal base of the nail bed and widens with time. Although this clinical sign isn’t an infallible predictor of a subungual melanoma, this is sufficiently concerning to me to warrant a referral to the dermatologist.
The above is similar to what I saw on Thursday afternoon. This concerned me, and thus I notified the GP about it. When he saw it, he confirmed my suspicion that this was indeed likely to be Hutchinson’s sign of the nail. He then promptly told the patient that he needed to consult a dermatologist to further manage this possibility of a subungual melanoma. There is a chance that what the patient has isn’t subungual melanoma, and I hope it isn’t but if it is indeed subungual melanoma, then at least having it promptly seen and managed by the dermatologist should render the prognosis more favourable.
“Good call”, the GP remarked to me.
I have never been more proud of myself. This encounter has reaffirmed my decision that was made more than three years ago to embark on a journey to become a medical doctor.
I hope my contribution as a medical student on Thursday potentially saved someone’s son, husband, and father.
NL
23 October 2021

Leave a comment