“Hey bro, do you have this thing called G6PD? What is this G6PD?” What do the title and the preceding sentence have in common? These are perhaps the words of full-time national servicemen, both 30 years ago and now respectively, to their fellow soldiers as they are left perplexed by the medical questionnaires they are tasked to complete.
Whilst serving in the SAF as a full-time national serviceman, I had the opportunity to go on overseas military training exercises. Before embarking on these overseas training trips, servicemen would need to ensure that they are certified to be medically fit for the relevant training. This would often entail getting the required vaccinations at the camp, declaring one’s vaccination history, and declaring any medical conditions to the senior medics or the medical officers at the medical centre of the army camp, either verbally or through the completion of forms.
I remember filling in some of these questionnaires and one of the points on these questionnaires would be:
“2. G6PD: Yes/No”.
I’m not even kidding. It was just this, word for word. Allow me to explain why such wording can technically be misinterpreted. Servicemen have to fill in these forms individually. A few weeks prior to leaving for training in Australia, my entire company was given such a form to fill in. In the company office, someone from another platoon asked one of the platoon commanders, “Sir, how do we fill this in? I’m not sure what G6PD is”. The lieutenant replied, “If you are not sure what it is, you probably don’t have it.”
On the surface, this seems to be a reasonable position to adopt. After all, if you have gotten through life this far without doctors ever having diagnosed you with G6PD (glucose 6-phosphate dehydrogenase) deficiency, you probably do not have the said condition. Here is an image of a patch that a soldier can put on his ILBV to indicate his G6PD deficiency:
Most students who have learnt of G6P (glucose 6-phosphate) first studied it in the context of glycolysis, gluconeogenesis, and glycogenolysis. However, the G6PD enzyme is relevant in neither of these pathways. Instead, it is an enzyme that is relevant to the pentose phosphate pathway/HMP (hexose monophosphate) shunt, which occurs in the cytosol. Now, this HMP shunt is quite important because it provides a source of NADPH from the available G6P. NADPH is used in reductive reactions such as glutathione reduction inside RBCs (red blood cells), fatty acid and cholesterol synthesis. Additionally, the shunt also yields ribose for nucleotide (those ATCGs in DNA) synthesis and glycolytic intermediates (fructose 6-phosphate and glyceraldehyde 3-phosphate). This is particularly important in RBCs because NADPH is needed to keep glutathione reduced, which in turn detoxifies free radicals and peroxides.
In other words, here are the pairs of redox reactions. Firstly, G6PD catalyses the irreversible oxidation of G6P to 6-phosphogluconolactone, which reduces NADP+ to NADPH.
NB: 6PGL (6-phosphogluconolactonase) then catalyses the oxidative hydrolysis of 6-phosphogluconolactone to give 6-phosphogluconate.
Next, NADPH is oxidised back to NADP+ when glutathione reductase catalyses the reduction of GSSG (glutathione disulfide) to 2 GSH (glutathione). NB: The ‘S’ and ‘H’ in GSSG and GSH represent sulfur and hydrogen atoms respectively. Lastly, 2 GSH is oxidised back to GSSG when glutathione peroxidase catalyses the reduction of H2O2 to 2 H2O.
I’m sure you can now clearly see the problem with having G6PD deficiency. When there is deficiency in G6PD, all the above reactions are inhibited. There won’t be as much NADPH produced, because there isn’t as much dehydrogenation from G6P to 6-phosphogluconolactone. Consequently, there would be hemolytic anaemia due to poor RBC defence against oxidising agents (remember the last step in the chain in the above paragraph where H2O2 is reduced to water; that now doesn’t occur as much). H2O2 is a reactive oxygen species that can be converted to hydroxyl radicals, which can attack the proteins in the cell.
Consider this quote from reference [4]:
“Protein oxidation is defined as the covalent modification of a protein induced either by the direct reactions with reactive oxygen species (ROS) or indirect reactions with secondary by-products of oxidative stress. ROS can cause oxidation in both amino acid side chains and protein backbones, resulting in protein fragmentation or protein-protein cross-linkages. Although all amino acids can be modified by ROS, cysteine, and methionine that are the most susceptible to oxidative changes due to high reaction susceptibility of the sulfur group in those amino acids. Oxidative modifications of proteins can change their physical and chemical properties, including conformation, structure, solubility, susceptibility to proteolysis, and enzyme activities.“
As the quote above says, amino acids with sulfur-containing R-groups are most susceptible to oxidative attack due to the relatively high reactivity of sulfur. Hence, it isn’t a surprise to learn that the hydroxyl radicals can attack haemoglobin in RBCs, causing a cross-linking of sulfhydryl groups on globin chains, which in turn causes haemoglobin to be denatured and precipitate. And what happens when oxidised haemoglobin precipitates?
Heinz bodies.
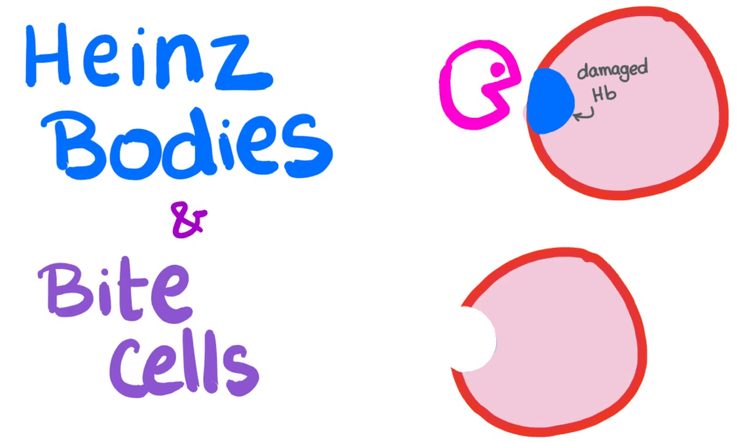
Look at this image above. That damaged haemoglobin coloured in blue represents a Heinz body. That pink Pac-man thing represents a splenic macrophage, which comes and “eats” the Heinz body. Bite cells, represented by the cell below the cell with the damaged haemoglobin, thus result from the phagocytic removal of Heinz bodies by splenic macrophages. Such original and creative naming. Lol.
G6PD deficiency is an X-linked recessive disorder, and is the most common human enzyme deficiency.
If we were to be quite pedantic, then the construct “2. G6PD: Yes/No” is, strictly speaking, problematic because it is people who are deficient in the enzyme G6PD that have the condition known as G6PD deficiency. In other words, people who have sufficient G6PD are fine and do not have G6PD deficiency. So, since normal people have G6PD, would it be wrong for people to circle “Yes”? On the other hand, the form is probably asking people whether they have the deficiency.
My recommendation to the SAF is to unambiguously alter the construct in the medical questionnaire to “G6PD deficiency: Yes/No”.
Personally, I wouldn’t be surprised if some people think that the “D” in G6PD means “deficiency”. After all, it doesn’t help that there is a practice where people repeat the full word of the last letter of acronyms (e.g. POP parade, IPPT test, PSLE exam, GUI interface, PIN number, ATM machine, D-Day, HIV virus, DC Comics, LCD display, OPEC countries).
Ironically, such a practice is known as RAS syndrome, where RAS stands for “redundant acronym syndrome”. What a term! For all who design invitation cards. please take note. Please don’t put “Please RSVP” on invitations!
Yours faithfully,
Nic Loh
23 May 2019
References & Further Reading
1. https://en.wikipedia.org/wiki/Pentose_phosphate_pathway
2. https://en.wikipedia.org/wiki/Fenton%27s_reagent
3. FA USMLE Step 1 2014.
4. https://www.ncbi.nlm.nih.gov/m/pubmed/24007423/

Leave a comment